When a program evaluates technology for vision care in the field, the question of clinical evidence rarely gets the weight it deserves.
Price gets a column in the spreadsheet. Portability gets a column. Battery life gets a column. But “how thoroughly has this device been validated, in what populations, under what conditions, and what did the research find?” is a harder question to reduce to a cell, so it often doesn’t get asked with the same rigor.
It should.
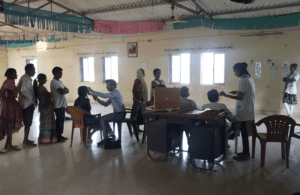
Clinical validation is not a formality. It is the record of how a device actually performs — on adults and children, in clinics and in the field, in India and Kenya and Spain and Brazil and the United States. It is the difference between a manufacturer’s specification and an independent finding. Between a promise and a proof.
QuickSee technology has been evaluated in 25+ IRB-based studies, with results published in Ophthalmology, BMJ Open Ophthalmology, Optometry and Vision Science, PLOS ONE, and Investigative Ophthalmology and Visual Science. The evidence base spans adult and pediatric populations, cycloplegic and non-cycloplegic conditions, clinic and field settings, across multiple countries and care contexts.
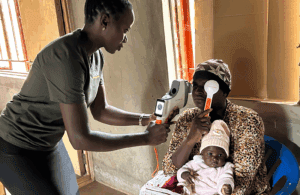
Two findings are worth singling out. In a 2024 validation study of QuickSee Free Pro in an adult population, the device’s measurement difference relative to subjective refraction was smaller than the variability between two subjective refractions performed by the same experienced clinician — suggesting measurement consistency comparable to the clinical gold standard itself. And in a 2019 comparison of three handheld autorefractors in a low-resource setting, QuickSee technology demonstrated the shortest learning curve for both practitioners and patients, and the most accurate measurements of the three devices evaluated.
Serious clinical capability is achievable in the field. The evidence base is how you know it — and how you hold manufacturers accountable for claims.