What does accuracy actually mean when you’re measuring thousands of people a year in the field?
It’s a fair question. “Accurate enough” is a phrase that appears in a lot of technology evaluations. It implies a spectrum, a sliding scale, a judgment call about acceptable error. And in low-resource settings, where every dollar and every hour matters, “accurate enough” can feel like a reasonable standard.
But accuracy isn’t abstract. It resolves into people.
In a 708-participant field study in rural India, minimally trained technicians used QuickSee technology to prescribe eyeglasses. The prescriptions were compared against those from experienced refractionists using standard subjective refraction.
Among patients forty and under — the majority of a typical field screening population — there was no statistically significant difference in prescription preference. The patients couldn’t tell which glasses came from which method.
That study is controlled proof of a principle we’ve seen hold across millions of people on six continents. QuickSee technology has been used at that scale because the research gave programs — and the clinicians leading them — the confidence that it would perform.
Every percentage point of measurement agreement that a program trades away in the name of cost savings resolves, at scale, into patients who received a prescription that was close — but not as good as it could have been. The question isn’t whether that matters in the abstract. It’s how many people per thousand you’re comfortable with.
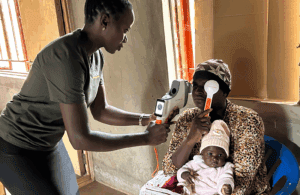
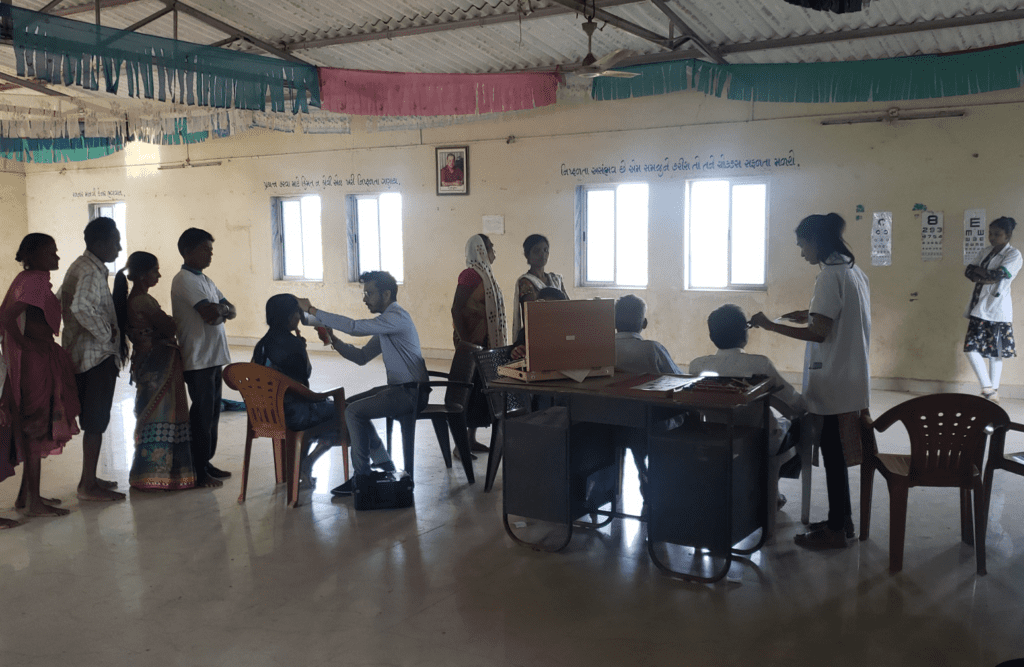
Accurate autorefraction in field settings isn’t a research finding. It’s a deployable standard. The Sarva Mangal Family Trust has been bringing it to people across India, Africa, and Southern California in their effort to reach 10 million patients and counting.
Photo: Local partners in the Sarva Mangal Family Trust (SMFT) initiative measure patients who gather at temporary exam sites where trained teams perform refraction and other eye health tests.