When we talk to NGO program leaders about technology selection for field vision care, we hear a version of the same assumption repeatedly: that in low-resource settings, some clinical compromise is inevitable. That accurate autorefraction is a clinic luxury. That the field demands a different — lower — standard.
We disagree. And we have the evidence to show why.
Over the past several posts we’ve made the case across four dimensions:
- That responsible technology selection weighs usability, accuracy, consistency, and clinical capability — not device price alone.
- That clinically accurate autorefraction at field scale is achievable — demonstrated in controlled research across hundreds of patients, with prescriptions that performed on par with those from experienced refractionists.
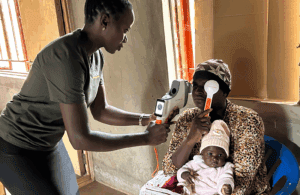
- That pediatric evaluation and myopia detection in the field is possible — QuickSee technology’s open-view design controls accommodation without cycloplegia, and the validation data in children support it.
- That the depth of clinical evidence is itself a selection criterion — 25+ IRB-based studies, published in Ophthalmology, BMJ Open Ophthalmology, PLOS ONE, and more, across multiple countries and patient populations.
QuickSee technology has now been used on millions of people in field settings worldwide. The controlled research isn’t the scale claim — it’s the proof that what we see at scale holds up under rigorous research conditions.
These are the conditions we designed QuickSee technology to meet, and they remain our guiding star. Not a clinical device adapted for rough environments. Not a compromise built to a price point. A system designed from the ground up to deliver the best possible autorefraction for anyone, anywhere — and validated to show it.
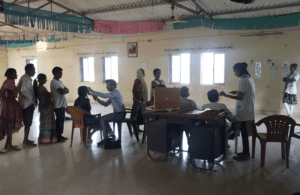
QuickSee Free Pro: handheld, battery-powered, calibration-free, no dark room required, operable by trained technicians. Deployed by programs serving millions of patients across six continents.
The tradeoff between clinical quality and field practicality is false. The standard exists. Programs can demand it.