Turn every screening into clinically actionable data.

Know exactly why — not just whether.
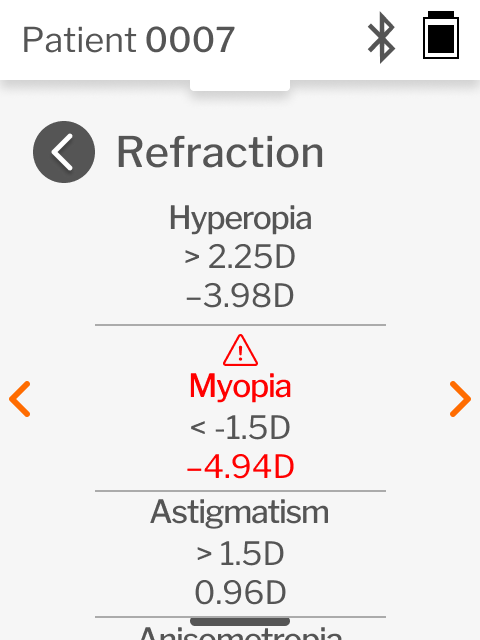
Most screeners return a binary pass/refer with no breakdown of what drove the result. QuickSee Free tells you which parameters triggered the flag, the measured values, and the thresholds applied. That’s the difference between a referral and actionable clinical data.
With an AUC of 0.95 for myopia detection (Bui et al., 2025) — the fastest-growing childhood vision condition — QuickSee Free’s wavefront technology delivers both pediatric screening accuracy and the clinical transparency providers need to act confidently.
Fast, accurate pass / fail feedback
Detailed clinical data on what caused screening failures
Not just a flag. A complete refraction picture.
Other screeners tell you who needs a workup. QuickSee Free gives the receiving clinician a head start: a comprehensive optical analysis of the eye — full wavefront-based refractive data, captured at the moment of screening. No starting from scratch. That’s what wavefront aberrometry — the same technology behind LASIK surgery planning — makes possible in a handheld device.
Clinical determinations remain with the eye care professional. QuickSee Free’s role is to make every referral better informed.

Built for the populations that need it most.
Schools, community outreach, mobile programs
Operates in any lighting — no dim room required, no calibration needed. The only device in its class that works reliably across the full range of real-world outreach environments.
Elder care and nursing home rounds
Full refraction and a triage result in a single step. When a resident is flagged, their complete refractive data is already captured — no second measurement needed, no re-examination in a difficult setting.
Mixed-age and general populations
Pediatric and adult-population guideline frameworks included. Screen children and adults in the same session without switching devices.
Diverse populations
Wavefront aberrometry is unaffected by iris pigmentation — a documented accuracy concern with photoscreeners in diverse communities.
Autorefraction you can trust.
Peer-reviewed clinical studies across adult and pediatric populations—including young children—demonstrate that objective refraction measurements obtained with QuickSee technology show strong agreement with subjective refraction and accuracy comparable to benchmark desktop autorefractors.
±0.25D
Excellent agreement: 70–75% of adult patients
Most precise threshold in clinical research
±0.5D
Good agreement: 80–90% of adult patients
Standard clinical threshold in
literature
Within ±0.50 D for astigmatic components
Precision on the hardest component to measure
Peer-reviewed results published in
How QuickSee Free compares to other screeners
| Feature | QuickSee Free | Welch Allyn Spot | PlusOptix |
|---|---|---|---|
| Refractive data at point of screening | Full wavefront-based data | Binary pass/refer only | Binary pass/refer only |
| Parameter-level flag breakdown | Yes | No | Partial |
| Iris pigmentation independence | Yes | No (sensitivity 0.78 light vs. 0.49 dark iris1) | Partial |
| Adult/mixed-age validated guidelines | Yes | No | No |
| Operates in any lighting | Yes | Yes | No — dim room required |
| 1 Pophal et al., 2024 | |||
Learn what QuickSee Free can do for your program
If you would like to see QuickSee Free in use, the next step is to schedule a demo or an on-site trial.
An on-site evaluation allows your team to assess refraction accuracy, workflow fit, and usability in your own care environment, with your patient population and staffing model.
QuickSee Free enables clinicians to perform refraction using objective measurements. Clinical judgment and comprehensive eye examinations remain the responsibility of the licensed provider.