Myopia is the fastest-growing cause of visual impairment worldwide. By 2050, half the world’s population is projected to be myopic. The majority of that growth is happening in children — and a significant portion of it in exactly the communities that field vision care programs serve.
This creates a measurement problem that doesn’t get enough attention in technology evaluations.
Children are harder to refract than adults. Accommodation — the eye’s ability to adjust focus — interferes with standard autorefraction in ways that are well documented and frequently underestimated. The conventional solution is cycloplegia: eye drops that temporarily paralyze the ciliary muscle and eliminate accommodative error. In a clinic, that’s a manageable protocol. In the field, it’s often impractical, time-consuming, and a barrier to the throughput that makes screening programs viable.
The question for field programs isn’t just whether a device works on adults in reasonable conditions. It’s whether it works on children, without cycloplegia, in the environments where those children actually live.
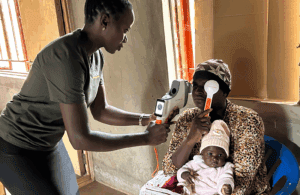
QuickSee technology was designed with an open-view measurement system that allows patients to fixate naturally during measurement. In children, this matters: natural viewing reduces accommodative effort in a way that conventional closed-view autorefractors cannot replicate. The result is more reliable measurements without the clinical overhead of cycloplegia.
The validation data support this. In a pediatric study comparing QuickSee technology against a desktop autorefractor, QuickSee performed better in children without cycloplegia — and visual acuity with QuickSee-derived corrections was equal to or better than subjective refraction in 74–77% of cases. In a separate pediatric clinical study, testability across ages three to seventeen exceeded 98%.
Hyperopes present a related challenge — and a related solution. Standard autorefraction tends to underestimate hyperopic refractive error. Open-view measurement, by reducing accommodation during the exam, produces a more complete optical picture of the hyperopic eye.
The hardest patients to measure accurately are often the ones a program can least afford to get wrong. The technology evaluation should account for that.