When vision care programs evaluate technology for field use, the conversation often starts with price. That’s understandable. Budgets are real. But price is one variable in a technology strategy — and not the most consequential one.
Consider what happens downstream when a program selects a device primarily on purchase cost. Measurements that are adequate in ideal conditions may be less reliable in the field. Children and hyperopes — populations that need accurate measurement most — may be systematically underserved by devices not designed for them. Prescriptions that are close enough in a controlled setting compound their error across thousands of patients and years of use.
This is not an argument that cost doesn’t matter. The total price difference between clinical accuracy and “close enough” across an entire program’s device fleet is measured in tens of thousands of dollars. The patient populations that difference is asked to serve are measured in the hundreds of thousands, or millions. The economics of compromise deserve the same scrutiny as the device price.
The question responsible programs should be asking isn’t: what is the lowest-cost device that will work?
It’s: how can technology help us meet our healthcare objectives?
Accurate autorefraction in field settings is not a luxury of the clinic. It is an achievable standard. Technology strategy criteria should reflect that.
Over the next few posts we’ll share the evidence — from peer-reviewed research, from pediatric validation studies, from programs operating at scale across six continents — that the responsible standard is real, and that settling for less is a choice, not a necessity.
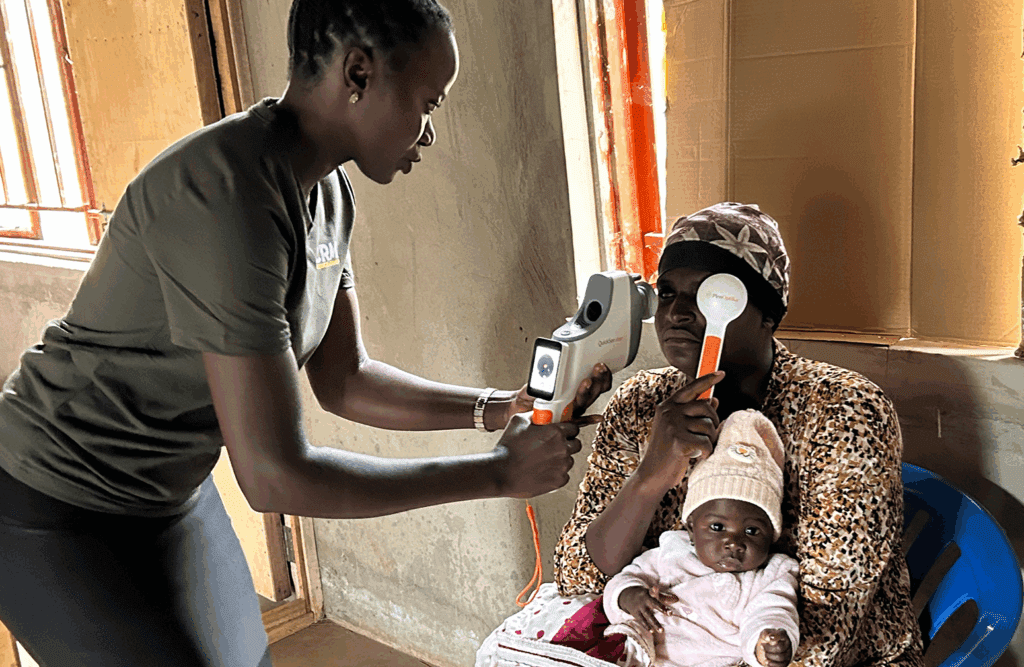
Shown above: Dr Randall Thomas’s mission to Uganda